Ridge Augmentation in Fair Lawn, NJ: Jawbone Rebuilding
Ridge augmentation in Fair Lawn, NJ rebuilds jawbone for strong dental implants. Learn more & contact Dental Professionals of Fair Lawn today.
Ridge augmentation in Fair Lawn, NJ rebuilds jawbone for strong dental implants. Learn more & contact Dental Professionals of Fair Lawn today.

Losing a tooth is stressful enough. Hearing that you're not ready for a dental implant yet because there isn't enough bone can feel like another setback.
That's a common moment for patients in Fair Lawn, NJ. Someone comes in expecting to talk about replacing a missing tooth, then learns the jawbone in that area has become too thin, too short, or too uneven to hold an implant the way it should. The good news is that this doesn't automatically close the door on implants. In many cases, it means the foundation needs to be rebuilt first.
For patients searching for a dentist near me, dental implants near me, or a dentist in Fair Lawn, NJ, understanding ridge augmentation can make that recommendation feel much less confusing. This procedure is about rebuilding the part of the jaw that supports a future implant, so the final result has a stronger base and a more natural shape.
A patient might come in after a past tooth extraction, ready to move forward with implant treatment, only to hear, “The bone isn't quite where we need it.” That's disappointing, especially when you've already spent time thinking about how nice it will feel to chew comfortably again and stop worrying about the gap in your smile.
In Fair Lawn, Ridgewood, and Glen Rock, many people are in that exact position. Bone loss after tooth loss is common. It doesn't mean treatment has failed. It means planning matters.
A dental implant needs support from healthy bone. If the ridge of bone is too narrow or too shallow, placing an implant right away can lead to a poor position, compromised support, or an unnatural-looking final tooth. Ridge augmentation helps rebuild that area before the implant goes in.
Much like setting a fence post, if the ground is too soft or the hole is too small, the post won't be stable no matter how well made the post is. The same idea applies here. The implant may be excellent, but it still needs enough healthy bone around it.
Ridge augmentation is often the step that turns “not yet” into “yes, you can be a candidate.”
Patients often assume a delay means something is wrong. Usually, it means your dentist is planning carefully. That's a good thing.
When a provider recommends rebuilding bone first, they're trying to give your implant a better long-term environment. That careful approach also fits into broader restorative dentistry goals, whether you're replacing one missing tooth or part of a larger treatment plan that may also involve cleaning and exams, dental x-rays, crowns, or other restorative care.
Ridge augmentation is a bone rebuilding procedure that restores the shape or volume of the jaw in an area where bone has been lost. The “ridge” is the part of the jawbone that used to hold the tooth root. After a tooth is removed or lost, that ridge can shrink.
A simple way to picture it is a house foundation. If you want to add a new room, you don't start with the walls or roof. You make sure the base underneath is wide and strong enough first. A dental implant works the same way. The visible crown is the part you see, but the implant underneath needs the right support.
When a tooth is no longer there, the body no longer has the same reason to maintain the surrounding bone in that exact shape. Over time, the area can become smaller. For some patients, that creates a ridge that's too thin for an implant. For others, it changes the gumline and contour enough that both function and appearance are affected.
That's why ridge augmentation is often part of treatment before implant placement. It rebuilds the site so the future tooth has a more secure and natural-looking base.
A clinical study gives a useful example of what that rebuilding can look like. After 6 months, mean ridge width increased from 3.14 ± 0.54 mm before augmentation to 6.71 ± 0.74 mm after augmentation in 20 augmentations performed in 15 patients, according to this 2024 ridge width study on lateral alveolar ridge augmentation.
Ridge augmentation isn't just “adding bone.” The goal is to create better dimensions for treatment that comes next.
That can include:
Later in the decision process, visual explanations can help. This short video gives a helpful overview before your consultation.
Practical rule: If the future implant needs a stable base, the bone has to be ready before the implant is placed.
For people looking into dental implants near me in Fair Lawn, this is often the missing piece of the conversation. You may not need to give up on implants. You may need to prepare the site properly first.
When patients hear they have “bone loss,” it can sound like one single problem. It isn't. The shape of that bone loss matters because it affects which treatment method makes sense.
The two descriptions you'll hear most often are horizontal defects and vertical defects.
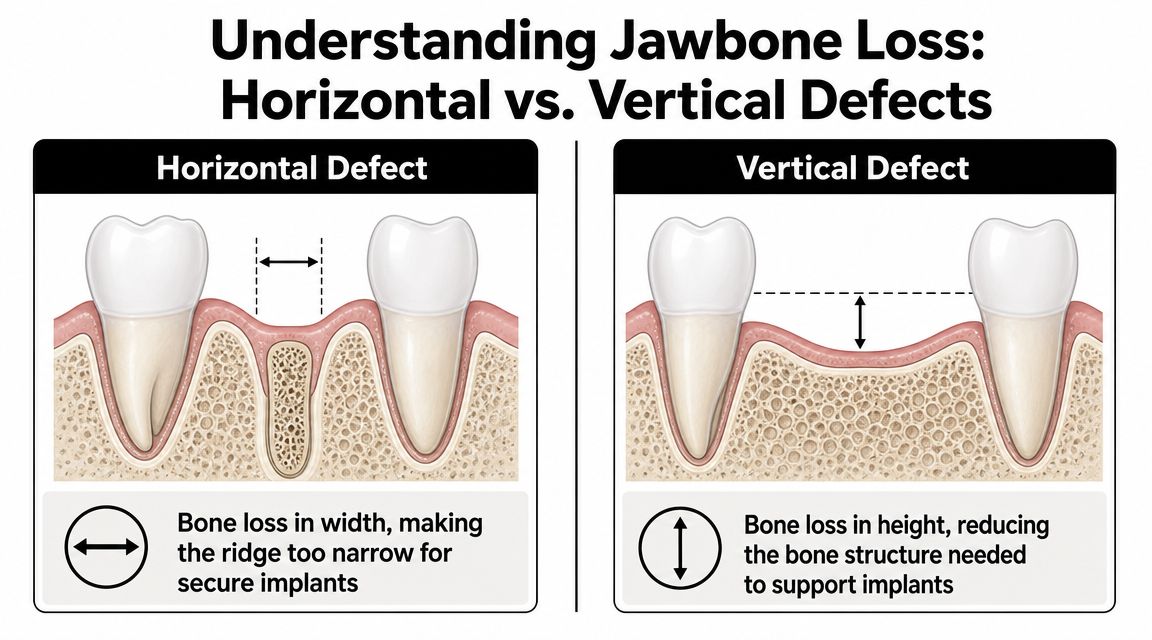
A horizontal defect means the ridge has lost width. In plain language, the bone is too narrow from side to side.
Patients often understand this quickly when you compare it to a shelf bracket. If the wall is too thin, there isn't enough structure to hold the bracket securely. An implant placed into a ridge that's too narrow may not have the surrounding bone it needs.
A vertical defect means the ridge has lost height. The bone may have enough thickness in one direction but not enough height to support ideal implant placement.
This tends to be harder for patients to picture because the gum may look fairly normal from the outside. But underneath, the bony support may sit lower than it should.
Some treatment decisions come down to one question. Is the site missing width, height, or both?
Ridge augmentation often requires a personalized approach. A thin ridge and a short ridge are not the same problem, so they usually don't call for the same exact solution.
The literature repeatedly points to this as an important gap in patient education. Ridge augmentation is often necessary for implant site development, but treatment choices vary by horizontal vs. vertical defects, and newer methods for vertical cases have been introduced to simplify treatment in selected situations, as discussed in this review of ridge augmentation approaches and defect-specific planning.
That's why a proper diagnosis matters so much. When patients understand whether their ridge is too thin, too short, or both, the recommendation stops sounding random and starts sounding logical.
You come in expecting to hear, "You need bone grafting," and instead you hear two or three possible approaches. That can feel confusing fast. The reason is simple. The technique is chosen to match the shape of your bone loss, not just the fact that bone loss exists.
In our Fair Lawn office, the conversation usually starts with one practical question. Does the site mainly need added width, added height, or stronger support to rebuild both safely for an implant?
Guided bone regeneration, or GBR, is often a good fit when the ridge needs more width or contour and the area can be rebuilt with particulate graft material protected during healing. A membrane is placed over the graft to hold the space and shield it while new bone forms.
A helpful way to picture GBR is as creating a protected healing chamber. The graft material gives your body a scaffold, and the membrane helps keep soft tissue from collapsing into that space too early. For many horizontal defects, that combination can work very well because the main goal is to make a narrow ridge wide enough to support an implant.
Technical details matter to your surgeon because grafts heal best when they stay stable and covered. For example, membrane extension and secure fixation are part of predictable treatment planning, as described in this guided bone regeneration protocol review. Patients do not need to memorize those steps. The bigger point is that protected, undisturbed healing gives the graft a better chance to turn into usable support for an implant.
Some defects need more than a contained layer of graft particles. If the ridge has lost a larger amount of structure, especially in height or in a very collapsed area, a block graft may be the better choice because it adds firmer physical support.
A block graft works like adding a solid frame before finishing a wall. Instead of filling a shallow depression, the surgeon is rebuilding a stronger outline where the ridge has become too reduced. This is one reason block grafting often enters the discussion for more demanding vertical defects or combined defects.
In some cases, the best graft material may include your own bone, called an autogenous graft. That option can be useful when biology and healing potential are a major part of the decision, such as defects with limited blood supply or sites that need a more active healing response. If your doctor recommends your own bone rather than only donor or synthetic material, the recommendation is usually based on what gives that specific site the best chance to heal into stable implant support.
A clear way to understand the recommendation is to focus on what the ridge is missing and what the technique is trying to accomplish.
| Technique | Often Chosen For | Why It May Fit |
|---|---|---|
| Guided bone regeneration | Many narrower ridges and contour deficiencies | Builds bone in a protected space when the site mainly needs added width or shape |
| Block grafting | More severe defects with structural loss | Adds firmer support where the ridge needs more substantial rebuilding |
| Autogenous graft-based approach | Challenging sites where healing biology is a major concern | Uses your own bone when the surgeon wants a graft source with strong regenerative potential |
Two patients can both need ridge augmentation and still receive very different recommendations. One person may have a ridge that is mostly too thin, where GBR makes sense. Another may have lost more height or support, where a block graft or an autogenous approach is more logical.
That difference is not arbitrary. It is the connection between your anatomy and the treatment plan.
If you want a broader, plain-language explanation of how grafting supports future implants, this article on bone grafting for dental implants explains the bigger picture. For patients choosing a dentist in Fair Lawn, NJ for implant treatment, one of the smartest questions to ask is, "Why does this technique fit my defect?" A good answer should connect the plan to your width, your height, your tissue condition, and the final implant goal.
Most patients want to know two things right away. How long will this take, and what will recovery feel like?
The honest answer is that ridge augmentation requires patience. Bone needs time to heal and integrate before an implant is placed into that area.
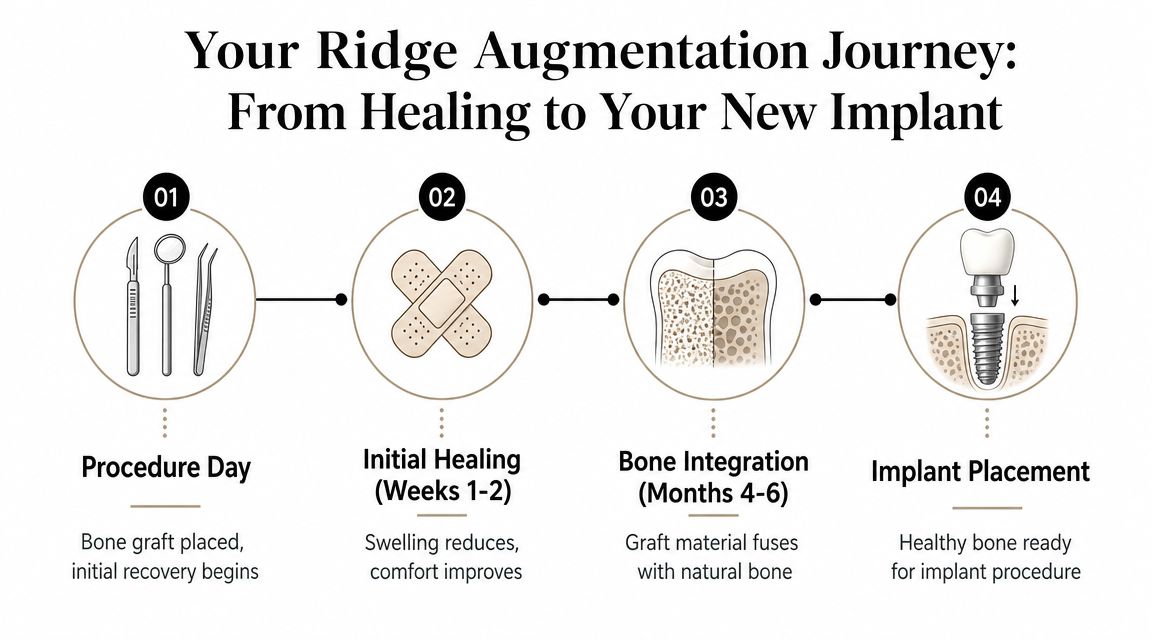
The procedure day is focused on rebuilding the site. After that, your body begins the early healing phase.
During the first part of recovery, patients are usually most focused on swelling, tenderness, eating carefully, and keeping the area clean without disturbing it. Soft foods are often the easiest choice while the area settles down. Careful home instructions matter because the graft needs a calm environment.
After the initial recovery, the primary work happens beneath the surface. The grafted site matures and integrates over time.
That waiting period is important because the goal isn't just to fill space. The goal is to create a site that can support the next phase of treatment. If you want to understand how this fits into the bigger sequence from consultation through final restoration, this overview of the dental implant timeline is helpful.
Healing time can feel slow when you're eager to finish treatment, but this stage is what gives the implant a stronger foundation.
Patients sometimes worry that a staged approach means uncertainty. In reality, careful site development is part of making implant treatment more predictable.
A retrospective implant study reported a 100% survival rate for implants placed in ridge-preserved sites, a related bone-preservation procedure performed at or shortly after extraction, as shown in this study on ridge preservation and implant outcomes. The same paper also reported overall success rates of about 51% in ridge-preserved sites versus about 58% in ungrafted sites, which is a reminder that survival and success are not identical measures and that each case still needs individualized planning.
This process asks for some patience. That part is real.
What helps most is knowing there's a purpose behind each step. You're not waiting because nothing is happening. You're waiting because your body is building the support the implant will rely on later.
Ridge augmentation makes sense when it solves a specific problem. The question is not merely, "Can I have this procedure?" The better question is, "Will rebuilding this area give me a better path to the tooth replacement I want?"
A good candidate is usually healthy enough for oral surgery, able to keep the area clean while it heals, and ready to follow instructions closely. Gum health matters. Smoking matters. The condition of the nearby tissue matters too, because bone grafting heals best in a stable, healthy environment.

Patients usually are not focused on the name of the procedure. They want to know what it helps them do.
Ridge augmentation can:
One simple way to think about it is foundation first, replacement second. If the bone is missing, the implant plan has to adapt. Sometimes that means rebuilding the area now so the final result is stronger and more natural later.
The reason for choosing augmentation often becomes clearer once the defect is identified.
A patient with a horizontal defect has lost width. In that situation, treatment may be recommended because there is not enough side-to-side bone to fully surround an implant. A patient with a vertical defect has lost height, which can make treatment more complex because the missing support is not just thinner bone, but taller bone that is no longer there. Some patients have both.
That difference matters because it affects the recommendation. A narrower ridge may respond well to one approach, while a taller or more advanced defect may call for a different grafting method or a more cautious treatment sequence. This is often the point where the plan starts to feel more personal. The choice is based on your anatomy, not a one-size-fits-all formula.
Ridge augmentation is one option, not the only option.
Depending on the timing and the condition of the site, alternatives may include:
Sometimes the decision is straightforward. If the missing bone is the main reason an implant is not possible, augmentation may be the most direct way to change that. In other cases, another treatment may fit your goals better, especially if you want to limit surgery, shorten treatment, or postpone implant care.
The right consultation should help you weigh those choices calmly. If you came in because of a broken tooth, a recent extraction, or an urgent problem, the first decision is often about what gives you the best long-term options, not just the fastest short-term fix.
When you come in for a ridge augmentation consultation, the first priority is clarity. Patients need to know what the bone looks like, why treatment is being recommended, and what the likely sequence will be from surgery to final restoration.
That planning often includes modern imaging, including 3D CBCT scanning, because implant-related bone treatment depends on seeing the shape of the site accurately. A ridge that looks acceptable in a simple two-dimensional view may tell a different story when width and height are evaluated more precisely.
For many patients, the bigger barrier isn't the technical part. It's anxiety.
That's why comfort planning matters just as much as surgical planning. Sedation dentistry can be part of the conversation for patients who feel nervous about oral surgery or who've delayed treatment because of fear. In a setting where various services are available, that can also make it easier to coordinate related services such as new patient exams, dental x-rays, restorative care, or future implant appointments under one broader care plan.
Dr. Jody Bardash brings 30+ years of experience to patient care. Just as important, patients need communication they can understand.
A good consultation should answer questions like these in plain language:
For adults looking for a new dentist near me in Fair Lawn, NJ, those conversations matter. So does having access to broader services in one practice, whether you're also interested in cosmetic dentist near me, Invisalign, Six Month Smile, or general family dental care.
If ridge augmentation has been mentioned in your treatment plan, the next step is a consultation that turns uncertainty into a clear path forward.
Patients usually leave the educational part of this topic with a few practical questions still on their mind. The table below addresses the ones that come up most often in real conversations.
| Question | Answer |
|---|---|
| Is ridge augmentation painful? | Most patients are more comfortable than they expected, especially when local anesthesia and, when appropriate, sedation are part of the plan. After the procedure, soreness and swelling are usually the main concerns, and your aftercare instructions are designed to help protect the area while it heals. |
| How long before I can get my implant? | It depends on the defect and the treatment approach. Some cases need a dedicated healing period before implant placement because the grafted area has to mature first. Your timeline should be based on your anatomy, not a one-size-fits-all schedule. |
| Will I need to miss work? | Many patients plan for a short period of reduced activity after surgery. The exact downtime varies by the size of the grafted area and the complexity of treatment. |
| Can ridge augmentation be done after a tooth has been missing for a long time? | Yes, in many cases it can. Older sites may require more rebuilding than a freshly treated extraction site, but a long-missing tooth does not automatically rule out treatment. |
| Is this the same thing as a regular bone graft? | Ridge augmentation is a type of bone grafting focused on rebuilding the tooth-bearing ridge so it can better support an implant and proper contour. |
| Will insurance cover it? | Coverage varies by plan and by how the treatment is categorized. The best way to get a reliable answer is to have the office review your benefits and provide a treatment estimate. |
| What if I'm nervous about oral surgery? | That's very common. Many patients do well once they understand the steps, know what sensations to expect, and discuss sedation options in advance. |
| Are there alternatives if I don't want ridge augmentation? | Sometimes yes, sometimes no. The answer depends on how much bone is missing, where it's missing, and what type of tooth replacement you want. A consultation should include alternatives whenever they are reasonable. |
If you're comparing options for restorative dentistry, dental implants, or care after a tooth extraction, questions like these are worth bringing to your visit. The right plan should make sense to you before treatment begins.
If you've been told you may not have enough bone for implants, a consultation can help you understand what's happening and what your options are. Dental Professionals of Fair Lawn provides implant planning, bone grafting, sedation dentistry, and a wide range of dental care for patients in Fair Lawn, Ridgewood, Glen Rock, and nearby New Jersey communities. Schedule a visit to find out whether ridge augmentation is the step that can move your treatment forward.